










Treatment
ACL Injury: Does It Require Surgery?

The following article provides in-depth information about treatment options for anterior cruciate ligament (ACL) injuries. It covers surgical techniques, rehabilitation, potential complications, and outcomes. It does not discuss knee anatomy, or the causes, symptoms, and diagnosis of ACL injuries. These topics are covered in the article Anterior Cruciate Ligament (ACL) Injuries, which we recommended you read before this article.
This information is intended to better inform patients about the management of ACL injuries.
Grades of ACL Tears
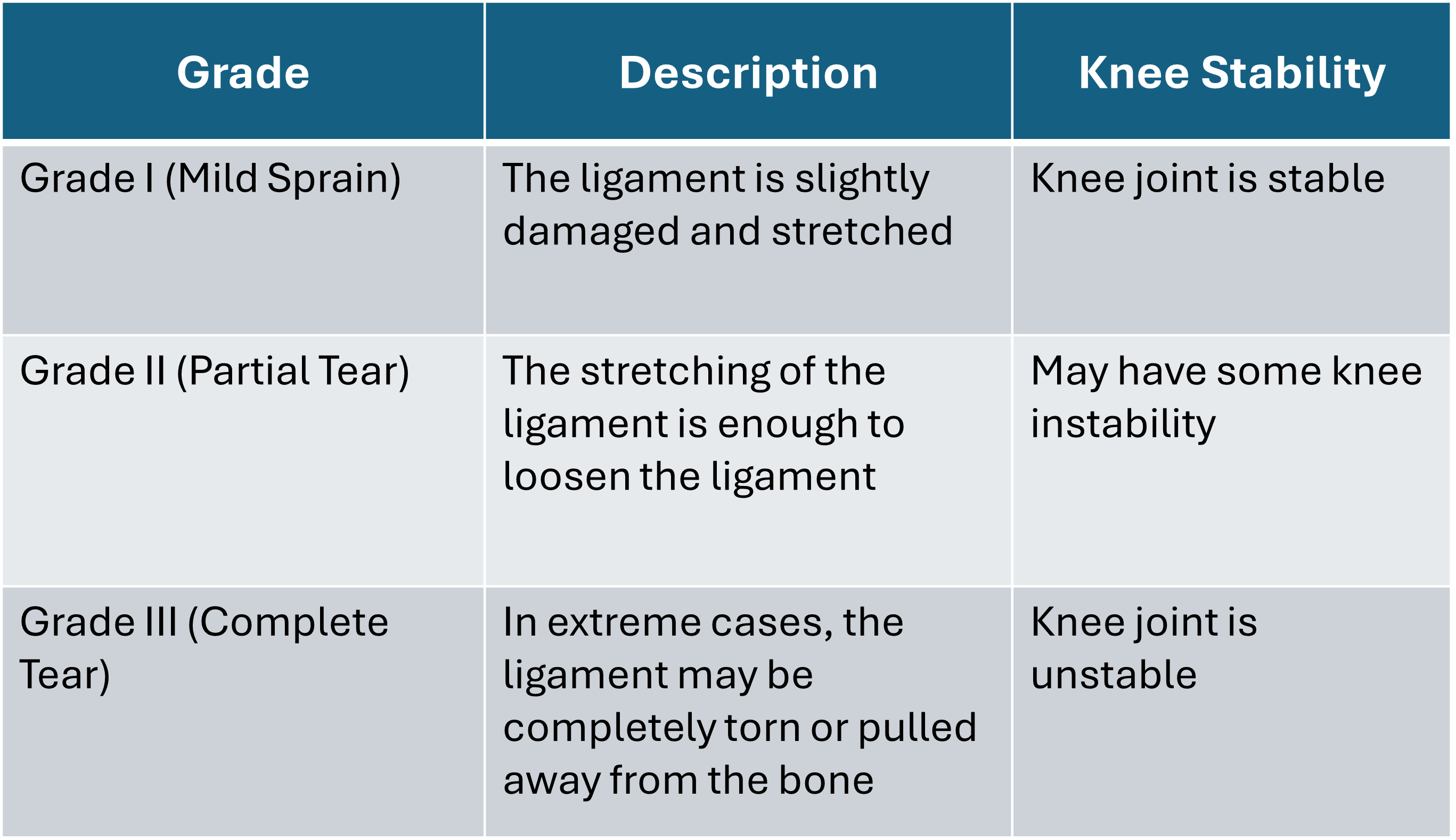
Partial tears of the anterior cruciate ligament are rare; most ACL injuries are complete or near complete tears.

Treatment of ACL Tears
The natural progression after an ACL injury varies from patient to patient. Treatment depends on:
- The patient's activity level
- The severity of the injury
- The degree of knee instability
- Whether there are other injuries, such as tears to other ligaments or the meniscus
Partial ACL Tears
Partial tears may be treated non-operatively with progressive physical therapy and rehabilitation.
The prognosis for a partially torn ACL can be good for low-intensity activity because the knee can be stable. The recovery and rehabilitation period usually lasts at least 3 months.
However, some patients with partial ACL tears may still have instability symptoms due to laxity (looseness) of the ACL. Close clinical follow-up and a complete course of physical therapy help identify those patients with unstable knees due to partial ACL tears.
Complete ACL Tears
Complete ACL tears typically have a less favorable outcome with non-operative management because of "perceived knee instability." That means the patient feels as if their knee is loose, weak, or might give way. Therefore, complete tears usually require surgical reconstruction.
- After a complete ACL tear, the perceived instability varies.
- Some patients feel instability during normal activities, such as walking.
- Others only notice the instability during cutting or pivoting sports.
- Rarely, patients can participate in sports without any symptoms of instability.
This variability is related to the severity of the injury, the strength of the surrounding muscles, and, most important, the type of sport(s) the patient plays.
About half of ACL injuries occur in combination with other injuries, such as meniscus tears, damage to articular cartilage (the smooth cartilage that covers the ends of bones), or tears of other knee ligaments.
Even if there is no meniscal injury at the time of the ACL injury, a majority of patients with chronic (long-standing) knee instability will develop a meniscal injury over the next few years. Articular cartilage lesions are also more common in patients who have a chronic ACL deficiency.
Nonsurgical Treatment of ACL Tears
The decision between nonsurgical treatments and surgery depends on multiple factors, including:
- Your activity level
- How soon you saw a doctor after the injury happened
- The presence of other injuries
- Your treatment goals
Progressive physical therapy and rehabilitation can restore the knee to a condition close to its pre-injury state and teach the patient how to prevent instability. The doctor may also recommend wearing a knee brace for added support. However, many people who choose not to have surgery suffer an injury to another part of the knee due to instability in the joint.
Who should consider nonsurgical management
Deciding against surgery is reasonable for certain patients. Nonsurgical management of isolated ACL tears is likely to be successful or may be recommended:- For patients with partial tears and no instability
- For patients with complete tears who don't experience symptoms of knee instability during activities and do not participate in pivoting or cutting sports
- For patients who do light manual work or live sedentary (inactive) lifestyles
For an acute isolated ACL tear, the American Academy of Orthopaedic Surgeons (AAOS) recommends 12 weeks of non-operative treatment and, if appropriate, performing surgery within 5 months to prevent any additional meniscus and chondral damage.
Surgical Treatment of ACL Tears
Surgical treatment is usually recommended for combined injuries (ACL tears that occur along with other injuries in the knee).
Following an ACL tear, the ACL is generally reconstructed rather than repaired. This is because the ACL, even when repaired, has a poor blood supply and is surrounded by joint fluid. This makes it difficult for the ACL to heal within the knee joint, causing a high failure rate of ACL repair.
Some patients may be candidates for ACL repair, possibly with biologic augmentation (e.g., platelet-rich plasma or bone marrow aspirate concentrate). These patients may have partial ACL injuries with instability, be lower-demand patients, or have an avulsion of the ACL off of its insertion on the femur (thigh bone).
You can discuss this option with your surgeon after you have an MRI and your doctor evaluates your condition to see if you fit the criteria.
The torn ACL is generally reconstructed using a substitute graft made of tendon. There are two types of graft:
- Autograft (grafts from the patient themselves)
- Patellar, hamstring, or quadriceps tendon autograft
- Allograft (grafts from a tissue donor)
- Patellar tendon, Achilles tendon, semitendinosus, gracilis, or posterior tibialis tendon allograft
Who Should Consider ACL Reconstruction Surgery?
- Active adult patients who are involved in sports or jobs that require pivoting, turning, or hard-cutting, or who perform heavy manual work are encouraged to consider surgical treatment. This includes older patients who have previously been excluded from consideration for ACL surgery. Activity level, not age, should determine whether surgery should be considered.
- In young children or adolescents with ACL tears, early ACL reconstruction creates a possible risk of growth plate injury, leading to bone growth problems. However, there is increasing evidence that children with ACL tears have a high risk of future damage to the meniscus or cartilage with nonsurgical treatment. Recent studies support early ACL reconstruction using alternative techniques that avoid the growth plate. Talk to your child's surgeon about the risks and benefits of surgery.
- A patient with a torn ACL and functional instability has a high risk of developing damage in other areas of the knee and should therefore consider ACL reconstruction.
- It is common to see ACL injuries combined with damage to the menisci, articular cartilage, collateral ligaments, joint capsule, or a combination of these structures. The "unhappy triad," frequently seen in football players and skiers, consists of injuries to the ACL, the medial collateral ligament (MCL), and the medial meniscus. In cases of combined injuries, surgical treatment may be necessary and generally produces better outcomes. Many meniscus tears are fixable, and they may have a higher healing rate if the repair is done at the same time as the ACL reconstruction.
Pain Management
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain.
Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Opioids can provide excellent pain relief; however, their use has risks and complications. These medications can be addictive and potentially dangerous. It is therefore important to use opioids only as directed by your doctor, to use as little as possible for as short a time as possible, and to stop taking them as soon as your pain starts to improve. Tell your doctor if your pain has not begun to improve within a few days after surgery.
Rehabilitation
Physical therapy is a crucial part of successful ACL surgery, with exercises beginning immediately after the surgery. Much of the success of ACL reconstructive surgery depends on the patient's dedication to rigorous physical therapy. With new surgical techniques and stronger graft fixation, current physical therapy uses an accelerated course of rehabilitation.
Post-operative course. In the first 7 to 10 days after surgery, the wound is kept clean and dry, and early emphasis is placed on regaining the ability to fully straighten the knee and restore quadriceps control.
The knee is iced regularly to reduce swelling and pain. The surgeon may order the use of a post-operative brace and a machine to move the knee through its range of motion, although this machine has not been shown to significantly improve patient outcomes.
Weightbearing status (use of crutches to keep some or all of the patient's weight off of the surgical leg) is also determined by physician preference, as well as other injuries addressed at the time of surgery.
Rehabilitation. The goals for rehabilitation of ACL reconstruction include:
- Reducing knee swelling
Maintaining mobility of the kneecap to prevent anterior knee pain problems or stiffness - Regaining full range of motion of the knee
- Strengthening the quadriceps and hamstring muscles
The patient may return to sports when:
- There is no longer pain or swelling
- They have achieved full range of motion in the knee
- Muscle strength, endurance, and functional use of the leg are fully restored
- Sense of balance and control of the leg are fully restored (through exercises designed to improve neuromuscular control).
Most patients are allowed to return to full sports participation within 6 to 12 months, depending on the patient's progress, strength, and mechanics.
The use of a functional brace when returning to sports is not necessarily required after a successful ACL reconstruction, but some patients may feel a greater sense of security by wearing one.
Potential Surgical Complications
Infection. The risk of infection after arthroscopic ACL reconstruction is very low. There have also been reported deaths linked to bacterial infection from allograft tissue due to improper procurement and sterilization techniques.
Viral transmission. Allografts specifically are associated with risk of viral transmission, including HIV and Hepatitis C, despite careful screening and processing. The chance of obtaining a bone allograft from an HIV-infected donor is calculated to be less than 1 in 1 million.
Bleeding, numbness. Rare risks include bleeding from acute injury to the popliteal artery, and weakness or paralysis of the leg or foot. It is not uncommon to have numbness of the outer part of the upper leg next to the incision, which may be temporary or permanent.
Blood clot. Although rare, a blood clot in the veins of the calf or thigh is a potentially life-threatening complication. A blood clot may break off in the bloodstream and travel to the lungs, causing pulmonary embolism or to the brain, causing stroke.
Instability. Chronic instability due to rupture or stretching of the reconstructed ligament or poor surgical technique is possible. It occurs in 5 to 10% of patients, long-term.
Stiffness. Knee stiffness or loss of motion has been reported by some patients after surgery and sometimes needs to be addressed surgically. The surgeon will either resect (remove) scar tissue or manipulate the knee under anesthesia.
Extensor mechanism failure. Rupture of the patellar tendon (patellar tendon autograft) or patella fracture (patellar tendon or quadriceps tendon autografts) may occur due to weakening at the site where the graft was harvested (removed).
Growth plate injury. In young children or adolescents with ACL tears, early ACL reconstruction creates a possible risk of growth plate injury, leading to bone growth problems. ACL surgery can be delayed until the child is closer to reaching skeletal maturity; however, this comes with a risk of future meniscus or cartilage injury. Alternatively, the surgeon may be able to modify the ACL reconstruction technique to decrease the risk of growth plate injury during surgery.
Kneecap pain. Post-operative pain in the front of the knee is common after patellar tendon autograft ACL reconstruction. The incidence of pain behind the kneecap varies greatly in studies. The incidence of kneeling pain is often higher after patellar tendon autograft ACL reconstruction.
To assist doctors in the management of anterior cruciate (ACL) ligament injuries, the American Academy of Orthopaedic Surgeons has conducted research to provide some useful guidelines. These are recommendations only and may not apply to every case. For more information: Plain Language Summary - Clinical Practice Guideline - Anterior Cruciate Ligament Injury - AAOS
Contributed and/or Updated by
Peer-Reviewed by
AAOS does not endorse any treatments, procedures, products, or physicians referenced herein. This information is provided as an educational service and is not intended to serve as medical advice. Anyone seeking specific orthopaedic advice or assistance should consult his or her orthopaedic surgeon, or locate one in your area through the AAOS Find an Orthopaedist program on this website.