










Diseases & Conditions
Hook of the Hamate Fracture of the Wrist
A hook of the hamate fracture is a break in one of the small bones (carpal bones) of the wrist. This type of fracture typically occurs during trauma to the palm and is associated with sports requiring the athlete to grip the handle of a piece of equipment (golf club, baseball bat, tennis racquet, etc.). Baseball and softball catchers can also sustain these fractures.
Symptoms of a hook of the hamate fracture typically include swelling and pain in the small finger side of the palm just past the wrist joint. Grasping, pushing, and pulling often makes the pain worse.
Treatment for a hook of the hamate fracture can range from immobilization (cast/or splint) to surgery. Optimal treatment can depend on the fracture's severity (how bad the break is), symptoms, and desire to return to previous activity (e.g. sports).
Anatomy
The wrist is formed by the two bones of the forearm — the radius and the ulna — and eight small carpal bones. The carpal bones are arranged in two rows at the base of the hand. There are four bones in each row.
The hamate bone is one of the carpal bones on the small finger side of the wrist, just above the ulna. The bone connects the wrist to the hand, specifically supporting the metacarpal bones of the ring and small (pinky) finger.
The hook of the hamate is a bony projection (a piece of the bone that sticks out). It extends from the hamate bone toward the palm. The hook is located in the middle of the palm slightly off center, toward the small (pinky) finger and just past the wrist crease.

The hook of the hamate has many attachments (ligaments and/or tendons that attach to a bone), but the most important is the transverse carpal ligament. This ligament extends from the hook of the hamate toward the carpal bones on the thumb side of the wrist.
Passing under the transverse carpal ligament (some quite close to the hook of the hamate) are:
- The tendons that connect to the fingers and thumb
- The median nerve, which supplies motor signal to some muscles of the thumb and feeling to the thumb, index finger, middle finger, and half of the ring finger
On the opposite side of the hook of the hamate (small finger side), the ulnar artery and ulnar nerve pass closely by.
- The ulnar artery is a major blood supply to the hand.
- The ulnar nerve supplies motor signal to many of the muscles of the hand as well as feeling to the small finger and half of the ring finger.
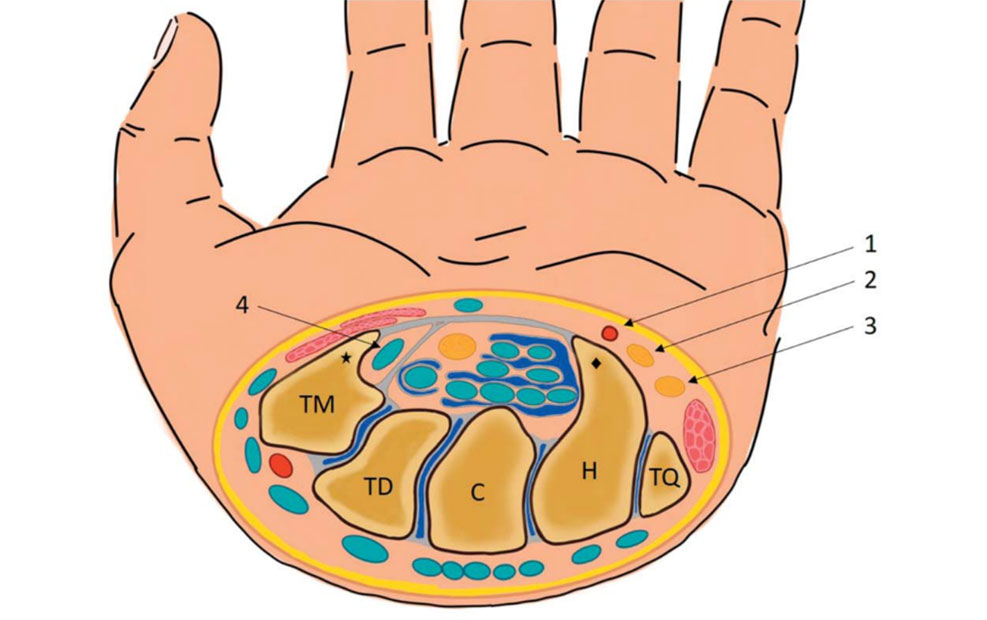
Because important structures (finger tendons on the thumb side, and the ulnar artery and nerve on the small finger side) run close by the hook of the hamate, they can be damaged during hook of the hamate fractures.
Furthermore, when hook of the hamate fractures do not heal, the jagged edges of the fracture can scrape and wear away these structures (particularly the tendons) and result in ruptures. This can make it difficult or impossible to pull the fingers down into the palm, such as when you are trying to grasp something or make a fist.
Description
Hook of the hamate fractures can be described by how close they are to where the hook actually arises (protrudes, or sticks out) from the rest of the hamate, though many fractures occur at the base of the hook.
Hook of the hamate fractures can also be classified according to the severity of displacement — how far the piece of bone has moved out of its normal position:
- Non-displaced fracture. In this type of fracture, the bone fragments line up correctly.
- Displaced fracture. In this type of fracture, the bone fragments have moved out of their normal position.

Cause
Hook of the hamate fractures typically occur due to trauma to the palm. This could include a fall, an object striking the palm, a motor vehicle collision, etc.
Classically, hook of the hamate fractures occur in athletes who grip the handle of a piece of equipment during sports like tennis (or other racquet sports), golf, and baseball. In these cases, the energy of the equipment striking the ball travels through the handle and breaks the hook of the hamate.

Fractures of the hook of the hamate typically occur in adults but can happen in people of all ages. There are no specific risk factors or diseases that make you more likely to experience a hook of the hamate fracture.
Symptoms
- Hook of the hamate fractures typically cause pain in the center of the palm a little closer to the small (pinky) finger side than to the thumb side and just past the wrist crease.
- The pain is typically made worse by grasping, pushing, and any other form of pressure over the palm.
Pain can be relatively mild and may be confused with a wrist sprain. As a result, many patients delay seeing a doctor. Some patients don’t see a doctor until they experience a complication of the fracture, such as a tendon rupture resulting in the inability to bring the finger into the palm.
Pain in your wrist/palm that does not go away within 1 day of the injury may be a sign of a fracture — so it is important to see a doctor if your pain does not go away. Prompt treatment of a hook of the hamate fracture may help avoid potential complications.
Doctor Examination
Medical History and Physical Examination
During the exam, your doctor:
- May talk with you about your general health
- Will ask how your injury happened
- Will ask you to describe your symptoms
Your doctor will also examine your wrist. With most fractures, there will be tenderness directly over the hook of the hamate in the palm. Your doctor will also look for:
- Swelling
- Bruising
- Loss of motion
Imaging Tests
X-rays. X-rays provide images of dense structures, such as bone. Your doctor will likely order an X-ray to help determine whether you have a hook of the hamate fracture and whether the broken pieces of bone are displaced. An X-ray will also help your doctor determine if you have any other fractures or dislocations.
In some cases, a hook of the hamate fracture does not show up on an X-ray. In those cases, more advanced imaging may be needed.
Computerized tomography (CT) scan. A CT scan can be helpful in revealing a fracture of the hook of the hamate and can also show whether the bone is displaced. Your doctor may use information from the CT scan to help determine your treatment plan.
Magnetic resonance imaging (MRI) scan. Your doctor may order an MRI to learn more about the bones and soft tissues in your wrist. An MRI can sometimes show a fracture of the hook of the hamate that cannot be seen on X-ray or even a CT scan.
Treatment
The treatment your doctor recommends will depend on several factors, including but not limited to:
- The location of the break in the bone
- Whether the bone fragments are displaced
- How long ago your injury happened
- Your age and general health
Nonsurgical Treatment
Hook of the hamate fractures can sometimes be successfully treated without surgery. Typically, treatment includes immobilizing the wrist in a cast or splint and avoiding activity that may disrupt fracture healing, such as grasping, pushing, and pulling.
Healing time varies from patient to patient. Your doctor will monitor your healing with X-rays or other imaging tests.
In some cases, your doctor may recommend the use of a bone stimulator to assist in fracture healing. This small device delivers low-intensity ultrasonic or pulsed electromagnetic waves that stimulate healing. Some early studies suggest that these devices may help the hook of the hamate to heal.
Surgical Treatment
Hook of the hamate fractures are often treated surgically for a variety of reasons.
- Athletes who demand a prompt return to sport may request surgery to speed up their recovery.
- Patients treated non-operatively without success — meaning, conservative treatments did not improve symptoms and/or function — may choose to proceed with surgery.
While hook of the hamate fractures can sometimes be fixed with pins or screws, a majority of surgeries actually involve excision (removal) of the hook of the hamate instead of attempting to get it to heal.
In most cases, surgically removing the hook of the hamate:
- Reverses symptoms.
- Does not negatively affect hand and wrist function.
- Speeds up recovery since there is no waiting period for the bone to heal. Patients can return to activity as soon as their skin incision is healed. Thus, this is often the procedure of choice for athletes.
Recovery
Nonsurgical treatment may include multiple weeks to months of immobilization in a cast or splint. During this time, unless advanced activity is approved by your doctor, you should avoid the following activities:
- Lifting, carrying, pushing, or pulling more than 1 pound of weight
- Batting, hitting a tennis ball, golfing, or participating in any activity that requires you to grip a piece of sporting equipment
- Participating in contact sports
- Climbing ladders or trees
- Participating in activities with a risk of falling onto your hand, such as inline skating or jumping on a trampoline
- Using heavy machinery or machines/pieces of equipment that vibrate
- Smoking, which can delay or prevent fracture healing; it can also affect healing after surgery
Surgery to repair the hook of the hamate fracture with fixation (securing the pieces of bone together using pins or screws) may also require several weeks to months of immobilization and activity modification.
Hook of the hamate excision often allows return to activity after wound healing (3 to 4 weeks) after a short period of immobilization.
It is important to maintain full finger motion throughout your recovery period. Your doctor will provide an exercise program, and they may refer you to a trained hand therapist who will help you regain as much range of motion and strength in your wrist as possible.
Despite hand therapy and a great deal of effort by the patient during home therapy, some patients may not recover the same range of motion and strength that they had before their injury.
Complications
Nonunion
A bone that fails to heal is called a nonunion. Nonunions are relatively common in hook of the hamate fractures that are treated non-operatively.
If your hook of the hamate fracture does not heal, your doctor may consider more surgery.
Tendon Rupture
As mentioned above, an unhealed hook of the hamate fracture can result in ruptures to the nearby tendons, which affects the ability to bring the fingers into the palm
Surgical Complications
Due to the important structures near the hook of the hamate (nerves, blood vessels, and tendons), surgical complications can occur that result in dysfunction of these structures — meaning, they no longer function normally. This can lead to pain, cold intolerance, numbness, weakness, and poor hand function. However, these complications are rare.
Contributed and/or Updated by
Peer-Reviewed by
AAOS does not endorse any treatments, procedures, products, or physicians referenced herein. This information is provided as an educational service and is not intended to serve as medical advice. Anyone seeking specific orthopaedic advice or assistance should consult his or her orthopaedic surgeon, or locate one in your area through the AAOS Find an Orthopaedist program on this website.